Explore the visionary perspectives of the Spinogenix leadership team. Our articles provide industry insights and thought leadership on our pioneering of synaptic regenerative therapies.
In The Scientist: Regenerating Synapses Could Help Treat Neurodegenerative Diseases
March 2, 2026
In The Scientist: Regenerating Synapses Could Help Treat Neurodegenerative Diseases By Dr. Peter Vanderklish
Rethinking Alzheimer’s Treatment: It’s Time for a New Playbook in the Fight for Memory

December 1, 2025
Authored by Stella Sarraf, PhD CEO, Founder In September, we recognized World Alzheimer’s Month and championed the much-needed attention and awareness to one of the greatest health crises of our...
Insights from the failed Harmony Zygel Trial and hope on the horizon with Spinogenix’s SPG601

October 24, 2025
On September 24, 2025, Harmony announced that Zygel, a synthetic cannabidiol, missed the primary endpoint in its pivotal Fragile X trial. While the outcome was disappointing for many families in...
Restoring Synapses, Restoring Hope: A Conversation with Jerre Stead

September 17, 2025
When Stead Impact Ventures Board Chair Jerre Stead sat down with Dr. Stella Sarraf, founder and CEO of Spinogenix, their discussion centered on one shared belief: patients deserve more than...
Honoring Dwight Clark’s Legacy: A Conversation with Steve Young

September 2, 2025
At Spinogenix, stories of courage and perseverance drive our mission in developing the novel synaptic regenerative treatments to bring new hope to people living with ALS and other neurodegenerative...
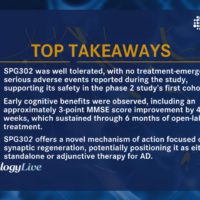
Findings From First Cohort of SPG302 in Phase 2 Alzheimer Disease Trial: Sharron Gargosky, PhD
August 1, 2025
Thank you to NeurologyLive for featuring, Dr. Sharron Gargosky, PhD, Chief Development Officer at Spinogenix, at the AAIC2025 in Toronto Sharron highlights key findings from our Phase 2a study on...
Restoring Synapses to Fight Neurodegeneration with Spinogenix CEO Dr. Stella Sarraf — Episode 217

July 30, 2025
Posted in Life Science Podcast By: Ayesha Rashid, PhD In this episode of the Xtalks Life Science Podcast, Ayesha speaks with Stella Sarraf, PhD, CEO and Founder of Spinogenix, a...
Spinogenix CEO and Founder Named to Forbes 50 Over 50: Innovation List

July 30, 2025
We’re thrilled to share that our CEO and Founder, Stella Sarraf, PhD, has been named to Forbes 2025 Class of 50 Over 50: Innovation list. This recognition celebrates trailblazers who...
This Founder Wants To Help Alzheimer’s Patients Restore Memory. Plus: Stop Spinning Your Wheels

May 2, 2025
By: Maggie McGrath, Forbes Staff andForbesWomen Team, Forbes Staff. Stella Sarraf founded drug discovery company Spinogenix in 2016 with a goal of finding a better way to treat neurodegenerative disorders—particularly Alzheimer’s...
A New Era in Schizophrenia Treatment: Dr. Christoph U. Correll on the Promise of SPG302
April 2, 2025
Spinogenix has reached a major milestone in its mission to transform neuropsychiatric care. Following FDA clearance of an IND application, enrollment is now open at a U.S. site for a...
Spinogenix Reports Positive Phase 2 Results for SPG601 in Fragile X Syndrome

March 10, 2025
Craig Erickson, MDChief Medical Advisor Spinogenix announced results from its Phase 2 study of SPG601, showing a strong efficacy signal in improving abnormal brain activity in Fragile X syndrome (FXS)....
Addressing the unmet need for synaptic regeneration in Schizophrenia
October 31, 2024
Craig Erickson, MDChief Medical Advisor Peter Vanderklish, PhDChief Science Office October marks the annual occurrence of several international events aimed at expanding awareness of mental health disorders, including schizophrenia. In...
Addressing Synaptic Deficits in Fragile X syndrome and how SPG601 could help
July 23, 2024
Craig Erickson, MDChief Medical Advisor July is Fragile X Awareness Month. We take this timely opportunity to hear our Chief Medical Advisor and Director of the Cincinnati Fragile X Research...
Synapse loss in Alzheimer’s disease and how SPG302 can help
June 20, 2024
Peter Vanderklish, PhDChief Science Officer June is Alzheimer’s and Brain Awareness Month. We take this timely opportunity to hear our Chief Science Officer, Dr. Peter Vanderklish, describe how SPG302 –...
Courage and Connections: Dan Doctoroff and Stella Sarraf Discuss ALS, Synapses, and Spinogenix’s Innovative Approach

June 12, 2024
By: Stella Sarraf, Ph.D., CEO and founder of Spinogenix Amyotrophic lateral sclerosis (ALS), commonly known as Lou Gehrig’s disease, was first described over 150 years ago. Despite decades of research,...
Using EEG and TMS to capture treatment-related Brain Signals in Spinogenix Drug Trials
February 6, 2024
Craig Erickson, MDChief Medical Advisor Drug development is a complicated, expensive, and time-consuming activity that requires thoughtful application of scientific and medical principles to bring the best possible treatments forward...